























Stefan Gleeson offers tools to help understand the impact of stress on individuals and teams.
So Abram said to Lot, "Let's not have any quarrelling between you and me, or between your herdsmen and mine, for we are close relatives. Is not the whole land before you? Let's part company."' (1)
'"Come now, let us settle the matter," says the LORD. "Though your sins are like scarlet, they shall be as white as snow; though they are red as crimson, they shall be like wool."' (2)
Conflict and arguments are commonplace - whether with a relative, colleague, or even with God. Reasons for such arguments range from irritability, due to long working hours, to personality differences and value clashes. As Christians our reactions are important not just because of relationships with others, but also in what they say to others about Jesus.
Dr Purple was three weeks into a new job. With a new contract threatening to eliminate her (already precarious) work-life balance, she asked her colleague, Dr Red, for advice. Dr Red was rude and abrupt. Dr Purple had to consider whether to: withdraw (and cope alone), go on the attack (pointed remark), or report to a senior (with potential long-term damage to relationship). What did she need to think about before reacting?
Here is a list of considerations; it is by no means exhaustive.
Team Environment: healthcare is becoming characterised by ongoing resource pressures in the face of rising demand. A drive to 'do more with less' leads to overstretched staff struggling to display compassion when emotionally overwhelmed. A single 'extra' demand on staff can lead to a less than professional response.
What of the doctor? Anthropological studies have found a tension between a doctor's need to become self-sufficient and the skills required for teamwork. (3) Competitive behaviour is often seen long after training is completed.
Consider which of the following zones characterises your team (bearing in mind that most teams will have gone through a red zone at some time). [See Box 1].
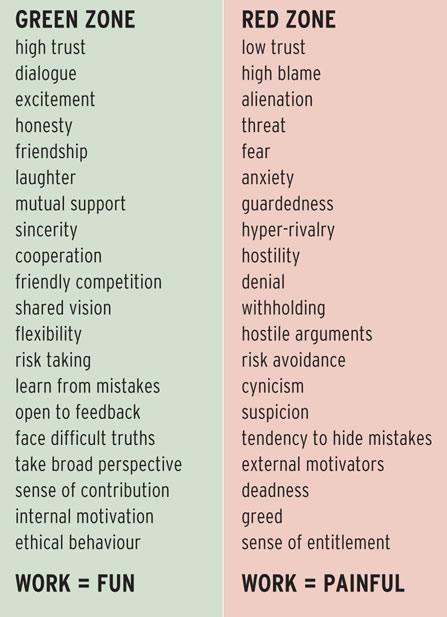 The GMC recognised the link between patient safety and learning environments last year. (5) Indeed, it is often medical students/trainees who raise concerns where red zone working is evident, but they can also point to areas of good practice: 'the environment was inquisitive, participatory rather than observation; not just about throughput' (Southampton Medical Student, 2014). There is evidence that Trusts, working with education providers, can turn work environments around. (6)
The GMC recognised the link between patient safety and learning environments last year. (5) Indeed, it is often medical students/trainees who raise concerns where red zone working is evident, but they can also point to areas of good practice: 'the environment was inquisitive, participatory rather than observation; not just about throughput' (Southampton Medical Student, 2014). There is evidence that Trusts, working with education providers, can turn work environments around. (6)
When Martha turned to Jesus, stressed that no one was helping her, we see in her a picture of the modern healthcare worker. Jesus told her that 'only one thing was needed'. (7) Role models are crucial in the development of future doctors, (8) so how we remain in Christ is essential if we are to influence teams for good. We should provide ethically responsive behaviour to challenges (saying sorry after an argument); take responsibility; be accessible, reliable, respectful, compassionate and self-appraising. We should aim to be wise doctors, 'nurturing the mind'. (9)
Secure in Christ, we work towards establishing effective teams, which are characterised by nondefensiveness, emotionally accessible care, constructive interaction, valuing others, situational (political and managerial) awareness, the ability to accept criticism and give people the benefit of doubt. (10)
Values: these are crucial to our motivation. The reason we went into medicine (hopefully) was to help people get better. The reality, in the current healthcare climate, is that our work is often beset with governance obligations - revalidation, ticking boxes to meet a standard (rather than formative development) and rota gaps. We can find ourselves reacting abruptly to competing demands when care is not patient-centred and resources are lacking. What can we do? We need to find ways to influence the political landscape (we cannot do this alone), but we also need to remember that we are human. Pablo Martinez writes of the duty of good stewardship in caring for our own wellbeing, or 'garden', in order to be able to look after others. (11)
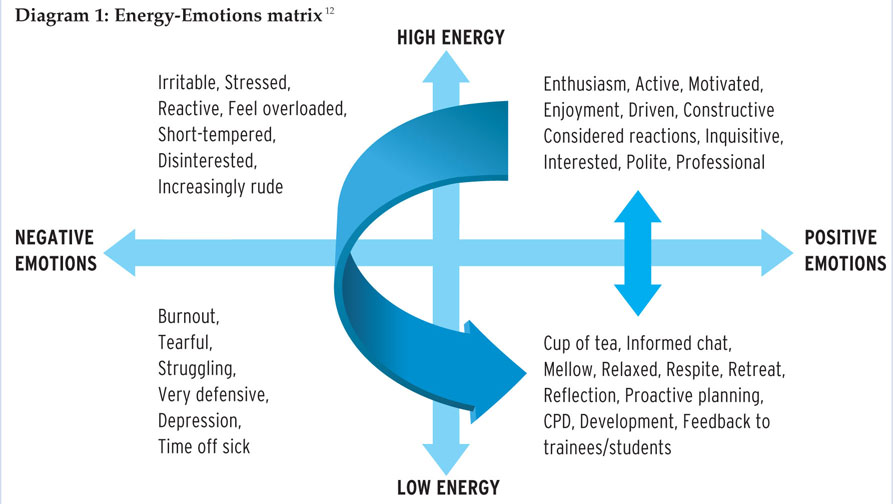
In the Energy-Emotions matrix below [Diagram 1], psychologists recognise that we can only last for two hours in the performance (top right) quadrant before either passively finding ourselves in survival mode (left top quadrant, characterised by stress) or proactively making a break to the recovery zone (bottom right). If we continue in stress/survival mode, we will burnout and be forced by sickness to return to the recovery zone. Jesus recognised this well when stretched by demand. He took himself regularly to a quiet place to reflect, pray and listen to his Father. (13)
Recognising the interaction between our vulnerabilities and stress
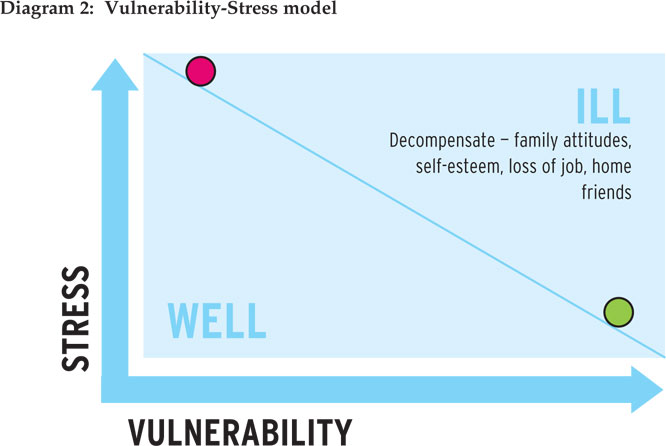
A Vulnerability-Stress model [Diagram 2] is one that may help us understand ourselves or our more challenging colleagues. It reflects the tipping point at which an additional level of stress overwhelms our coping mechanisms and health defences. It can help us understand why someone else may be stressed when we are not. Essentially, the more vulnerabilities (genetic, developmental, maturity) the more likely it is that even small sources of stress lead to illness. When ill, other factors may conspire to keep us ill (eg poor self-esteem). If we have few vulnerabilities (no family history of illness, great childhood), then it may still be possible to become unwell if we add sufficient stress.
Perception: our perception of others is affected by our own development, current health and circumstances.
Development: one in a hundred people have an autistic view of the world. The prevalence is higher among doctors, who might be unintentionally rude without noticing, not engage in small talk and need detailed instructions. A gentle but direct approach can work and a GP referral for a diagnosis can help autistic doctors understand themselves better. (15)
Current health and circumstances: in the UK between 25-76% of doctors experience burnout at some point in their career and up to 20% suffer from depression. (16) During acute stress, we are often preoccupied with the source (eg complaints) (17) so we find ourselves irritable with colleagues and/or emotionally exhausted with loss of concern for patients. Acute stress tends to resolve fairly quickly. However, depression, substance misuse and personality disorders need to be addressed via primary care. Finally, if home circumstances are difficult, colleagues may present with either absenteeism or presenteeism (avoiding home) from/at work.
How should we respond?
We need first to recognise that we have 'all have sinned and fall short of the glory of God'; (18) we are unable to manipulate others into change. 'Seek first to understand', (19) while maintaining boundaries (you are not there to please people). (20)
Secondly, recognise your resources: Jesus called us into our profession and wants us to bring the challenges to Him. We need to develop active listening skills to get to the heart of the matter. (21) The 'matter' may be to do with a mix of the 'challenging other person' (health, performance, culture) and/or our own 'challenging selves' (eg via 360 degree feedback). Improve your awareness of support organisations; share with mentors within your church/organisation and keep records.
Finally, we need to forgive others. (22) We are invited to 'ask God to bless everyone who ill-treats you. Ask Him to bless them and not to curse them'. (23) In the Sermon on the Mount, Jesus calls us to be peacemakers, to seek peace and pursue it but remember that if people do not want to live in peace with us, Jesus' instruction was qualified with 'if it is possible' and 'as far as it depends on you'. (24) The cost of peacemaking may involve 'painstaking listening, witnessing bitterness, apologising if we are to blame, making restitution'. (25) However, as John Stott says, 'always temper justice with mercy and mercy with justice'. (26)
Ultimately Jesus knew his disciples, and he will meet us where we are at. (27) As we deal with challenging colleagues and situations, He will remind us: 'Be still and know that I am God - I will be exalted among the nations'. (28)
Based on a seminar at the CMF National Conference in April 2016.







